Endometriosis
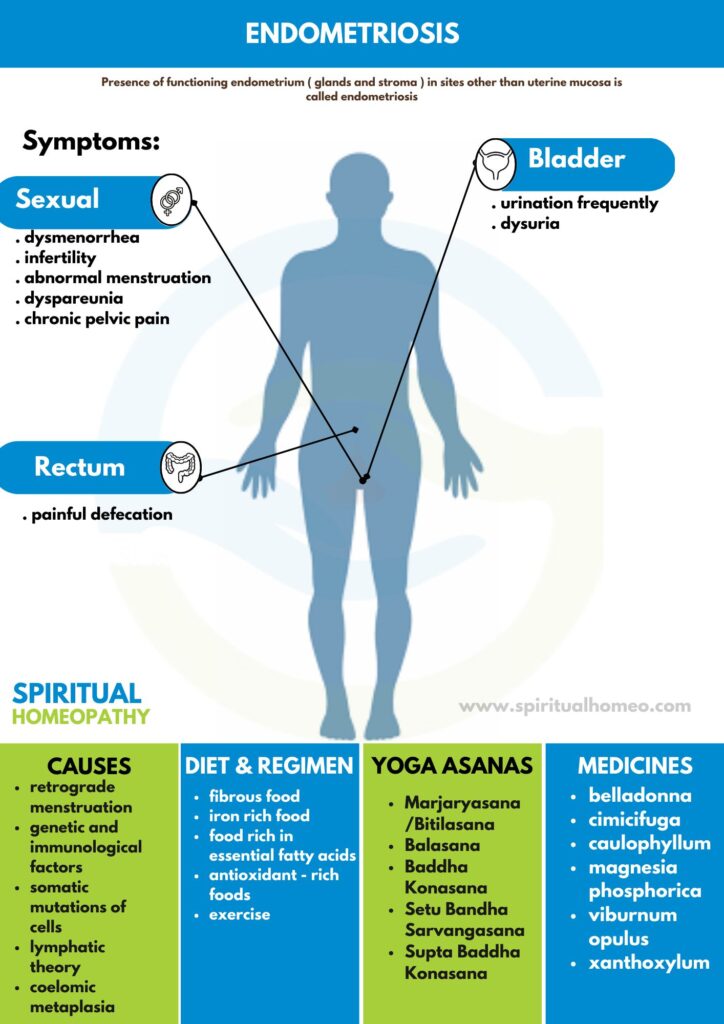
Presence of functioning endometrium (glands and stroma) in sites other than uterine mucosa is called endometriosis.
- Overview
- Causes
- Types
- Sign & Symptoms
- What to eat
- Diet and Regiment
- Homeopathic Treatment
- FAQ
- Reference
OVERVIEW
These ectopic endometrial tissues may be found in the myometrium when it is called endometriosis internal or adenomyosis. More commonly, however, these tissues are found at sites other than uterus and are called endometriosis externa or generally referred to as endometriosis.
Endometriosis is a disease of contrast. It is a benign but it is locally invasive, disseminates widely. Cyclic hormones stimulate growth but continuous hormones suppress it.
During the last couple of decades, the prevalence of endometriosis has been increasing both in terms of real and apparent. The real one is due to delayed marriage, postponement of first conception and adoption of small family norm. The apparent one is due to increased use of diagnostic laparoscopy as well as heightened awareness of this disease complex amongst the gynaecologists. The prevalence is about 10 percent. However, prevalence is high amongst the infertile women (30–40%) as based on diagnostic laparoscopy and laparotomy.
Sites:
- Abdominal
- Extra-abdominal
- Remote
Abdominal:
It can occur at any site but is usually confined to the abdominal structures below the level of umbilicus.
Extra-abdominal:
The common sites are abdominal scar of hysterotomy, caesarean section, tubectomy and myomectomy, umbilicus, episiotomy scar, vagina and cervix.
CAUSES
- Retrograde menstruation: In retrograde menstruation, menstrual blood containing endometrial cells flows back through the fallopian tubes and into the pelvic cavity instead of out of the body. These endometrial cells stick to the pelvic walls and surfaces of pelvic organs, where they grow and continue to thicken and bleed over the course of each menstrual cycle.
- Transformation of peritoneal cells: In what’s known as the “induction theory,” experts propose that hormones or immune factors promote transformation of peritoneal cells — cells that line the inner side of your abdomen — into endometrial-like cells.
- Embryonic cell transformation: Hormones such as estrogen may transform embryonic cells — cells in the earliest stages of development — into endometrial-like cell implants during puberty.
- Surgical scar implantation: After a surgery, such as a hysterectomy or C-section, endometrial cells may attach to a surgical incision.
- Endometrial cell transport: The blood vessels or tissue fluid (lymphatic) system may transport endometrial cells to other parts of the body.
- Immune system disorder.: A problem with the immune system may make the body unable to recognize and destroy endometrial-like tissue that’s growing outside the uterus.
TYPES
Endometriosis is also grouped by what area of the pelvis or abdomen it affects. There are four main types:
- Superficial peritoneal endometriosis: The peritoneum is a thin membrane that lines your abdomen and pelvis. It also covers most of the organs in these cavities. In this type, the endometrial tissue attaches to the peritoneum. This is the least severe form.
- Endometriomas: These are dark, fluid-filled cysts. They’re also called chocolate cysts. They vary in size and can appear in different parts of your pelvis or abdomen, but they’re most common in the ovaries.
- Deeply infiltrating endometriosis (DIE): In this type, the endometrial tissue has invaded the organs either within or outside your pelvic cavity. This can include your ovaries, rectum, bladder, and bowels. It’s rare, but sometimes a lot of scar tissue can bond organs, so they become stuck in place. This condition is called frozen pelvis. But this only happens to 1%-5% of people with endometriosis.
- Abdominal wall endometriosis: In some cases, endometrial tissue can grow on the abdominal wall. The cells may attach to a surgical incision, like one from a C-section.
SIGNS AND SYMPTOMS
Patient Profile
The age is between 30–45. The patients are mostly nulliparous or have had one or two children long years prior to appearance of symptoms. Infertility, voluntary postponement of first conception until at a late age and higher social status are often related. Thus, it is more common in private than hospital patients. There is often family history of endometriosis. Outflow tract obstruction is an important cause when it is seen in teenagers (10%)
Symptoms
- About 25 percent of patients with endometriosis have no symptom, being accidentally discovered either during laparoscopy or laparotomy.
- Symptoms are not related with extent of lesion. Even when the endometriosis is widespread, there may not be any symptom; conversely, there may be intense symptoms with minimal endometriosis.
- Depth of penetration is more related to symptoms rather than the spread. Lesions penetrating more than 5 mm are responsible for pain, dysmenorrhea and dyspareunia.
- Non-pigmented endometriotic lesions compared to the classic pigmented “powder burns” lesions produce more prostaglandin F (PGF) and hence are more painful.
- The symptoms are mostly related to the site of lesion and its ability to respond to hormones. Midline lesions are more symptom producing. Degree of pain is not related to the severity of endometriosis.
Dysmenorrhea (70%)
There is progressively increasing secondary dysmenorrhea. The pain starts a few days prior to menstruation; gets worsened during menstruation and takes time, even after cessation of period, to get relief of pain, (co-menstrual dysmenorrhea). Pain usually begins after few years pain-free menses. The site of pain is usually deep seated and, on the back, or rectum. Increased secretion of PGF 2α, thromboxane β2 from endometriotic tissue is the cause of pain.
Abnormal menstruation (20%):
Menorrhagia is the predominant abnormality. If the ovaries are also involved, polymenorrhagia or epimenorrhagia may be pronounced. There may be premenstrual spotting.
Infertility (40–60%):
Whether endometriosis causes infertility or infertility produces endometriosis is not clear.
Endometriosis is found in 20–40 percent of infertile women, where as in about 40–50 percent patients with endometriosis suffer from infertility. The multiple factors involved in producing infertility Dyspareunia
(20–40%)
The dyspareunia is usually deep. It may be due to stretching of the structures of the pouch of Douglas or direct contact tenderness. As such, it is mostly found in endometriosis of the rectovaginal septum or pouch of Douglas and with fixed retroverted uterus.
Chronic Pelvic Pain
The pain varies from pelvic discomfort, lower abdominal pain or backache. The cause may be multifactorial. These include—(i) Inflammation in the peritoneal implants and release of PGF, and also due to adhesions and ovarian cysts. (ii) Action of inflammatory cytokines released by the macrophages. (iii) Invasion of nerves or involvement of bladder and bowel. The pain aggravates during period.
Abdominal Pain
There may be variable degrees of abdominal pain
around the periods. Sometimes, the pain may be acute due to rupture of chocolate cyst.
Other Symptoms
The symptoms are related to the organ involved.
- Urinary—frequency, dysuria, back pain or even
haematuria
- Sigmoid colon and rectum—painful defecation (dyschezia), diarrhea, constipation, rectal bleeding or even melena
- Chronic fatigue, perimenstrual symptoms (bowel, bladder)
- Hemoptysis (rarely), catamenial chest pain
- Surgical scars—cyclical pain and bleeding
What to Eat for Endometriosis
Anti-inflammatory Foods – Turmeric, ginger, and garlic help reduce inflammation and ease symptoms.
Omega-3 Fatty Acids – Fatty fish (salmon, sardines), flaxseeds, and walnuts help lower inflammation.
Fiber-Rich Foods – Whole grains, beans, lentils, and vegetables aid digestion and hormonal balance.
Cruciferous Vegetables – Broccoli, cauliflower, and Brussels sprouts support liver detoxification of estrogen.
Iron-Rich Foods – Spinach, pumpkin seeds, and lean meats help counteract heavy bleeding.
Plant-Based Proteins – Tofu, legumes, and quinoa reduce red meat consumption, which may worsen symptoms.
Magnesium-Rich Foods – Bananas, almonds, and dark chocolate help with muscle relaxation and pain relief.
Hydrating Foods – Cucumbers, watermelon, and coconut water reduce bloating and inflammation.
Herbal Teas – Green tea and chamomile tea provide antioxidants and pain relief.
Avoid Processed & Sugary Foods – Reduce dairy, gluten, caffeine, and alcohol to prevent inflammation.
DIET AND REGIMEN
To fight inflammation and pain caused by endometriosis, it’s best to consume a nutrient-dense, well-balanced diet that’s primarily plant-based and full of vitamins and minerals. Add these to your diet:
- fibrous foods, such as fruits, vegetables, legumes, and whole grains
- iron-rich foods, such as dark leafy greens, broccoli, beans, fortified grains, nuts, and seeds
- foods rich in essential fatty acids, such as salmon, sardines, herring, trout, walnuts, chia, and flax seeds
- antioxidant-rich foods found in colorful fruits and vegetables, such as oranges, berries, dark chocolate, spinach, and beets
Make sure you pay attention to how your body acts when you eat certain foods. Keeping a journal of the foods you eat and any symptoms or triggers you have may be helpful.
Consider meeting with a registered dietitian. They can help you plan meals that work best with you and endometriosis, as there’s no one-size-fits-all approach.
Exercise:
Exercise may help with the management of endometriosis, too. This is because exercise can reduce estrogen levels and release “feel-good” hormones.
In addition to conventional methods of treatment, alternative treatments may be very helpful for women with endometriosis. For example, relaxation techniques may be beneficial. These can include:
- Meditation
- Yoga
- Acupuncture
- Massage
Why Choose Spiritual Homeopathy?
At Spiritual Homeopathy, we offer a unique approach to healing that integrates traditional homeopathic principles with a deep understanding of the spiritual aspects of health. Our team of experienced homeopathic practitioners combines expertise with empathy, ensuring that you receive the highest standard of care tailored to your individual needs.
Our Approach to Treatment
We believe that true healing occurs when all aspects of a person—physical, emotional, and spiritual—are in balance. That’s why our treatment approach goes beyond simply addressing symptoms to identify and treat the underlying imbalances contributing to your health concerns. By addressing the root cause of illness and supporting your body’s innate healing ability, we empower you to achieve lasting health and vitality.
Services We Offer
Consultations: Our experienced best homeopathy doctors in Hyderabad offer comprehensive consultations to assess your health concerns, medical history, and individual needs. we also take online consultation and We take the time to listen to your story, understand your unique health goals, and develop personalized treatment plans tailored to your specific needs.
Remedies: At Spiritual Homeopathy, we provide a wide range of homeopathic remedies carefully selected to address a variety of health conditions. From acute ailments to chronic diseases, our remedies are safe, gentle, and effective, offering natural relief without the side effects often associated with conventional medications.
Follow-Up Care: We believe in the importance of ongoing support and monitoring throughout your healing journey. Our team is dedicated to providing regular follow-up care to track your progress, adjust treatment as needed, and ensure that you are on the path to optimal health and well-being.
Our Commitment to You
At Spiritual Homeopathy, your health and wellness are our top priorities. We are committed to providing you with compassionate care, personalized treatment, and the support you need to achieve your health goals. Whether you are seeking relief from a specific health concern or simply looking to optimize your overall well-being, we are here to support you every step of the way.
FAQ
What is Endometriosis?
Presence of functioning endometrium (glands and stroma) in sites other than uterine mucosa is called endometriosis.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Endometriosis?
- Cimicifuga
- Caulophyllum
- Belladonna
- Viburnum opulus
- Xanthoxylum
- Magnesia
- Phosphorica
- Pulsatilla
- Cocculus
What causes Endometriosis?
- Retrograde Menstruation
- Coelomic metaplasia
- Direct implantation
- Lymphatic theory
- Genetic and immunological factors
- Environment theory
What are the symptoms of Endometriosis?
- Dysmenorrhea
- Abnormal menstruation
- Infertility
Dyspareunia
- Chronic Pelvic Pain
- Abdominal Pain
- Dysuria
- Haematuria
REFFERNCE
- DC Dutta Text book of Gynaecology
- Therapeutics from zomeo Ultimte LAN
- https://www.healthline.com/health/endometriosis/endometriosis-diet#exercise-and-alternative-therapies
Endometriosis
– Symptoms and causes – Mayo Clinic
Endometriosis : What Are the Types and Stages? (webmd.com)
Endometriosis physical examination – wikidoc
- Differential Diagnosis for Endometriosis: Similar Conditions
- How to Treat Endometriosis Naturally without Drugs (restartmed.com)