Botulism
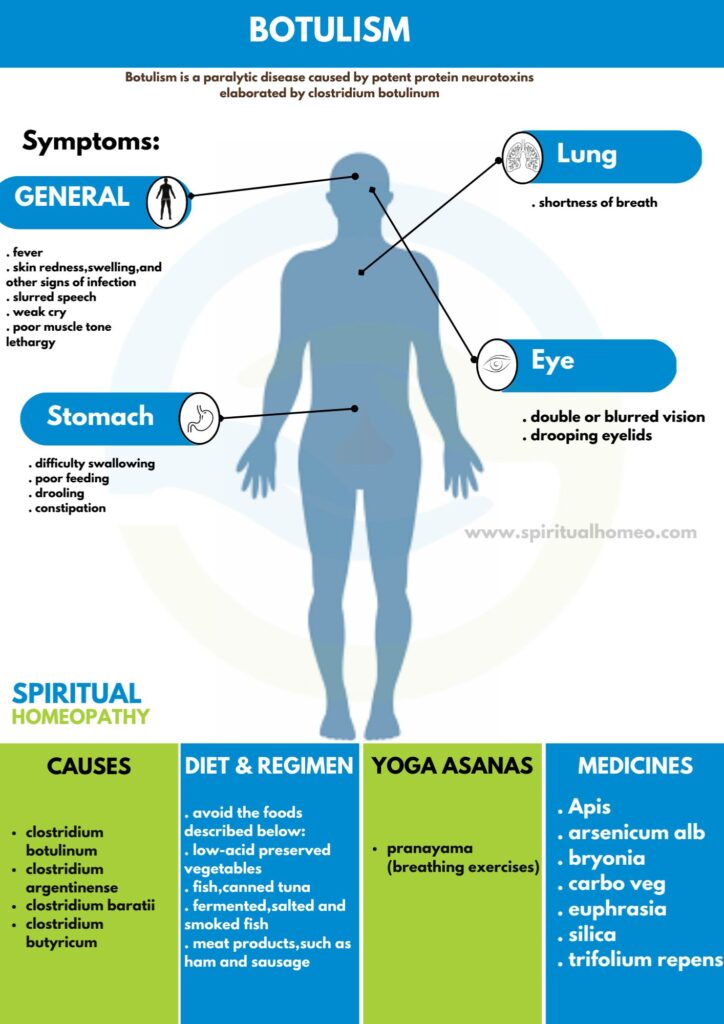
Botulism is a paralytic disease cause by potent protein neurotoxins elaborated by clostridium botulinum.
- Overview
- Causes
- Types
- Sign & Symptoms
- What to eat
- Diet and Regiment
- Homeopathic Treatment
- FAQ
- Reference
OVERVIEW
Botulismis recognized at least since the eighteenth century, is a neuroparalytic disease cause by botulinum toxin, one of the most toxic substances known. While initially thought to cause only by the ingestion of botulinum toxin in contaminated food (food-borne ofbotulism), three additional forms cause by in situ toxin production after germination of spores in either a wound or the intestine are now recognized worldwide: woundbotulism, infantbotulism, and adult intestinal colonizationbotulism.
In addition to occurring in these recognized natural forms of the disease, botulism’s symptoms have report in patients receiving injections of botulinum toxin for cosmetic or therapeutic purposes (iatrogenicbotulism). Moreover, botulism was reported after inhalation of botulinum toxin in a laboratory setting.
Spread of Botulism
All forms of botulism’s manifest as a relatively distinct clinical syndrome of symmetric cranial-nerve palsies followed by descending bilateral flaccid paralysis of voluntary muscles, which may progress to respiratory compromise and death. The mainstays of therapy are meticulous intensive care and treatment with antitoxin as soon as diease is suspected and before other illnesses have been ruled out.
Botulismoccurs worldwide, but the number of cases reported varies among countries and regions.
The variation may be due not only to actual differences in incidence but also to
(1) availability of resources to identify botulism, a rare disease
(2) differences in reporting requirements
(3) limited external access to data collections
There is no universal surveillance system to capture worldwidebotulism incidence. However, 30 countries currently participate in voluntary reporting ofbotulism cases to the European Union through an established surveillance system that includes standardized case definitions similar to those used in the United States and Canada. Other countries (e.g., Argentina, China, Thailand, Japan) maintain independent botulism surveillance.
CAUSES
Seven serologically distinct confirmed serotypes of botulinum toxin (A through G) have confirm. Botulinum toxin produce by four recognized species of clostridia: Clostridium botulinum, Clostridium argentinense, Clostridium baratii, and Clostridium butyricum. Certain strains may produce more than one serotype.
All are anaerobic gram positive organisms that form subterminal spores; C. botulinum and C. argentinense spores have recover from the environment. The spores survive environmental conditions and ordinary cooking procedures. Toxin production, however, requires a rare confluence of product storage conditions: an anaerobic environment, a pH of >4.6, low salt and sugar concentrations, and temperatures of >4°C. Although commonly ingested, spores do not normally germinate and produce toxin in the adult human intestine.
Food-borne botulism
Food-bornebotulism cause by consumption of foods contaminated with botulinum toxin; no confirmed host-specific factors involved in the disease. Woundbotulism cause by contamination of wounds with C. botulinum spores, subsequent spore germination, and toxin production in the anaerobic milieu of an abscess or a wound.
Infantbotulism
Infant botulism results from absorption of toxin produced in situ by toxigenic clostridia colonizing the intestine of children ≤1 year of age. Colonization thought to occur because the normal bowel microbiota not yet fully establish; this theory support by studies in animals. Adult intestinal colonization botulism, a very rare form that poorly understood, has a pathology similar to that of infant botulism but occurs in adults; typically, patients have some anatomic or functional bowel abnormality or have recently used antibiotics that may help toxigenic clostridia compete more successfully against the normal bowel microbiota.
Antitoxin treatment
Despite antitoxin treatment, relapse due to intermittent intraluminal production of toxin may observe in patients with adult intestinal colonization botulism. Regardless of how exposure occurs, botulinum neurotoxin enters the vascular system and transport to peripheral cholinergic nerve terminals, including neuromuscular junctions, postganglionic parasympathetic nerve endings, and peripheral ganglia.
Botulinum toxin is a zinc-endopeptidase protein of ~150 kDa, consisting of a 100-kDa heavy chain and a 50-kDa light chain.
Steps in neurotoxin activity include
(1) Heavy-chain binding to nerve terminals
(2) Internalization in endocytic vesicles
(3) Translocation of the light chain to cytosol
(4) Light chain serotype-specific cleavage of one of several proteins involved in the release of the neurotransmitter acetylcholine.
Inhibition of acetylcholine release by any of the seven toxin serotypes results in characteristic flaccid paralysis. Recovery follows sprouting of new nerve terminals.
Botulinum toxin serotypes
All botulinum toxin serotypes have demonstrated to cause botulism in nonhuman primates. Human cases associated with serotypes A, B, E, and F are reported each year. Serotype A produces the most severe syndrome, with the greatest proportion of patients requiring mechanical ventilation. Serotype B appears to cause milder disease than type A in both food-borne and infant botulism.
Other serotype
Besides this, Serotype E, most often associated with foods of aquatic origin, produces a syndrome of variable severity. The rare cases of illness caused by toxin serotype F, whether in infants or adults, characterize by rapid progression to quadriplegia and respiratory failure but also by relatively rapid recovery.
Recent studies have shown that at least some serotypes can be differentiated into subtypes through neurotoxin gene sequencing; however, the impact of these subtype differences on clinical illness is not yet known.
TYPES
Food borne botulism: –
From 1899 to 2011, 1225 food-borne botulism events (single cases or outbreaks) reported in the United States; from 1990 to 2000, a median of 23 cases were reported annually. Most such events (~80%) involve vegetables or fish/ aquatic animals, usually home-preserved (canned, jarred). Native communities in both the United States (Alaska) and Canada have a high incidence of food-borne botulism due to traditional food preparation practices; 85% of all cases in Canada occur in Native communities. Outbreaks typically involve two or three cases; however, one restaurant-associated outbreak in 1977 affected 59 persons.
Wound botulism: –
This form of disease first recognized in 1951 as a result of a review of the clinical records on an accidental injury in 1943. Between 1943 and 2011, 491 cases of wound botulism were reported in the United States; 97% of cases reported after 1990 were associated with injection drug use. The typical patient a 30- to 50-year-old resident of the western United States with a long history of black-tar heroin injection. In the early 2000s, wound botulism associated with drug use emerged in Europe, and at least two case clusters have reported.
Infant botulism: –
More than 3900 infant botulism cases have reported worldwide (84% in the United States alone) since this form of the disease first recognized in 1976; ~80–100 cases (commonly caused by serotypes A and B) reported annually in the United States.
Adult intestinal colonization botulism.: –
This form of botulism difficult to confirm because it is poorly understand and because no clear guidelines are available to help differentiate it from other adult botulism cases. Often these cases cause by C. baratii type F, but the involvement of both C. botulinum type A and C. butyricum type E has report.
Iatrogenic botulism: –
Paralysis of variable severity has followed injection of licensed botulinum toxin products for treatment of conditions involving hypertonicity of large muscle groups. The U.S. Food and Drug Administration received 658 reports of adverse events related to botulinum toxin use—some very serious—between 1997 and 2006. Although some patients had symptoms consistent with botulism, no cases laboratory confirmed. Injection of approved doses of licensed products for cosmetic purposes has not associated with botulism. However, four cases of laboratory-confirmed botulism resulted from illegal injection of research-grade toxin for cosmetic purposes in a U.S. medical facility in 2004
Inhalational botulism: –
Inhalational botulism does not occur naturally. One report from Germany has described botulism resulting from possible inhalational exposure to botulinum toxin in a laboratory incident.
Intentional botulism: –
Botulinum toxin has been “weaponized” by governments and terrorist organizations. An attack might use aerosolization of toxin or contamination of foods or beverages ranging in scope from small-scale tampering to contamination of a widely distributed food item. An unnatural event may be suggested by unusual relationships between patients (e.g., a visit to the same building), atypical exposure vehicles, or atypical toxin serotypes.
No matter how you get botulism, the symptoms are usually the same. The most defining symptom is weakness that starts on both sides of your face, goes down to your neck, and then to the rest of your body.
SIGNS AND SYMPTOMS
No matter how you get botulism, the symptoms are usually the same. The most defining symptom is weakness that starts on both sides of your face, goes down to your neck, and then to the rest of your body.
Other early symptoms e.g.:
- Either Double or blurred vision
- Drooping eyelids
- Difficulty swallowing
- Slurred speech
- Shortness of breath
Other symptoms that can follow include vomiting, belly pain, and diarrhea. Later, you may have a very hard time urinating and have severe constipation. Symptoms do not include a fever.
If you don’t get treatment, your symptoms could progress to paralysis of your arms and legs and the muscles used for breathing.
Infants with botulism have symptoms that i.e.:
- Lethargy
- Poor muscle tone starting in the head and neck and moving down
- Poor feeding
- Drooling
- Weak cry
Symptoms of wound botulism
Symptoms of wound botulism are similar to general botulism but may take about 2 weeks to appear. They also can i.e.:
-
Fever
- Skin redness, swelling, also other signs of infection
Symptoms of inhalation botulism
Symptoms of inhalation botulism are the same as those for general botulism but usually happen more quickly. Respiratory failure can occur.
Symptoms of adult intestinal toxemia
Symptoms of adult intestinal toxemiaare similar to infant botulism. They are the same as general botulism but may also include i.e.:
- Firstly, Constipation
- Secondly, Poor feeding
- Lastly, Lack of energy (lethargy)
Symptoms of iatrogenic botulism
Symptoms of iatrogenic botulism are the same as those seen in general botulism. Along with muscle weakness, you could have i.e.:
- Eye muscle weakness
- A hard time speaking
- A paralyzed face
- A thick, weak tongue
- Reduced gag reflex
Cranial nerve deficits i.e.
- Diplopia, Dysarthria
- Dysphonia, Ptosis
- Ophthalmoplegia
- Facial paralysis
- Impaired gag reflex
- Pupillary reflexes may be depressed, also fixed or dilated pupils
- Autonomic symptoms such as dizziness, dry mouth, and very dry, occasionally sore throat are common.
-
Constipation
- Respiratory failure may occur due to either paralysis of the diaphragm and accessory breathing muscles or pharyngeal collapse secondary to cranial nerve paralysis
- Weakness descends, often rapidly, from the head to involve the neck, arms, thorax, and legs; occasionally, weakness is asymmetric.
- Deep tendon reflexes may be normal or may progressively disappear.
Other symptoms
- Paresthesias, while rare, have been reported and may represent secondary nerve compression from immobility due to paralysis.
- Absence of cranial nerve palsies or their onset after the appearance of other true neurologic symptoms makes botulism highly unlikely.
- Nausea, vomiting, and abdominal pain may precede or follow the onset of paralysis in food-borne botulism.
- Infants with botulism typically present with reduced ability to suck and swallow, constipation, weakened voice, ptosis, sluggish pupils, hypotonia, and floppy neck; as in adults, illness can progress to generalized flaccidity and respiratory compromise.
WHAT TO EAT
To support metabolism, focus on foods that provide steady energy and boost metabolic processes. Include lean proteins like chicken, fish, and tofu to support muscle mass, which helps burn more calories. Whole grains like oats, quinoa, and brown rice provide complex carbohydrates, ensuring a slow, consistent energy release. Healthy fats from avocados, nuts, and olive oil help maintain hormone balance. Fruits and vegetables like berries, spinach, and broccoli are rich in antioxidants and vitamins, supporting overall health. Drink plenty of water and green tea, as hydration and caffeine can also enhance metabolic function. Regular meals and snacks are key for keeping metabolism active.
DIET AND REGIMEN
Must avoid this type of food:
- The botulism toxin has found in a variety of foods, including low-acid preserved vegetables. For example; green beans, spinach, mushrooms and beets; fish, including canned tuna, fermented, salted and smoked fish. Besides this; meat products, such as ham and sausage
HOMEOPATHIC TREATMENT
Why Choose Spiritual Homeopathy?
At Spiritual Homeopathy, we offer a unique approach to healing that integrates traditional homeopathic principles with a deep understanding of the spiritual aspects of health. Our team of experienced homeopathic practitioners combines expertise with empathy, ensuring that you receive the highest standard of care tailored to your individual needs.
Our Approach to Treatment
We believe that true healing occurs when all aspects of a person—physical, emotional, and spiritual—are in balance. That’s why our treatment approach goes beyond simply addressing symptoms to identify and treat the underlying imbalances contributing to your health concerns. By addressing the root cause of illness and supporting your body’s innate healing ability, we empower you to achieve lasting health and vitality.
Services We Offer
Consultations: Our experienced best homeopathy doctors in Hyderabad offer comprehensive consultations to assess your health concerns, medical history, and individual needs. we also take online consultation and We take the time to listen to your story, understand your unique health goals, and develop personalized treatment plans tailored to your specific needs.
Remedies: At Spiritual Homeopathy, we provide a wide range of homeopathic remedies carefully selected to address a variety of health conditions. From acute ailments to chronic diseases, our remedies are safe, gentle, and effective, offering natural relief without the side effects often associated with conventional medications.
Follow-Up Care: We believe in the importance of ongoing support and monitoring throughout your healing journey. Our team is dedicated to providing regular follow-up care to track your progress, adjust treatment as needed, and ensure that you are on the path to optimal health and well-being.
Our Commitment to You
At Spiritual Homeopathy, your health and wellness are our top priorities. We are committed to providing you with compassionate care, personalized treatment, and the support you need to achieve your health goals. Whether you are seeking relief from a specific health concern or simply looking to optimize your overall well-being, we are here to support you every step of the way.
FAQ
What is Botulism
Botulism a paralytic disease caused by potent protein neurotoxins elaborated by clostridium botulinum.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Botulism
- Arsenicum album
- Carbo veg
- Apis
- Bryonia
- Euphrasia
- Trifolium Repens
What are the symptoms ofBotulism
- Double or blurred vision
- Drooping eyelids
- Difficulty swallowing
- Slurred speech
- Shortness of breath
-
Vomiting, belly pain, diarrhea
What are the causes of Botulism
Clostridium botulinum
- Clostridium argentinense
- Clostridium baratii
- Clostridium butyricum
REFFERNCE
[1]Harrisons_Principles_of_Internal_Medicine-_19th_Edition-_2_Volume_Set
[2]https://www.webmd.com/food-recipes/food poisoning/what-is-botulism
[3] A Complete Repertory of The Tissue Remedies of Schussler by S. F. Shannon
[4], clinical examination